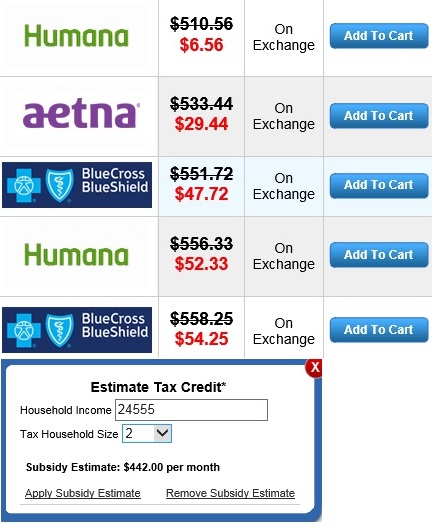
If you live in Ohio you can click on this calculator below to figure out your subsidy.
If you are low income, under $250 a week, click here to see some options.
- If you get a subsidy you will need help to process your application.
- Once you determine your subsidy you will have to visit Help Me Get My Health Insurance Plan.
If you get a subsidy you will need help to process your application.
- Once you determine your subsidy you will have to visit Help Me Get My Health Insurance Plan.
*All assistance provided is no cost to you. Purchasing a plan through Obamacare / the Federal Exchange is not the best option for everyone. A Health Insurance Plan Comparison and Consultation will be the best way for individuals and families to find affordable Ohio health insurance and see all their options.
If you only need dental coverage. Visit Ohio Dental Insurance.
NOTICE: It is important to understand the ACA eliminates medical underwriting. A person’s height and weight or pre-existing conditions do not affect one’s health insurance premium.





