New Super Reward Benefits for 2024. $0 Copay Plans. Learn more about your coverage options. Get $0 Deductible, $0 Copay, and My Health Pays Rewards Cards.


New Super Reward Benefits for 2024. $0 Copay Plans. Learn more about your coverage options. Get $0 Deductible, $0 Copay, and My Health Pays Rewards Cards.

Need a Quote or have a question about Ambetter Health Insurance? We are here to assist with shopping, enrolling or renewing your 2023 Ambetter Health Insurance:
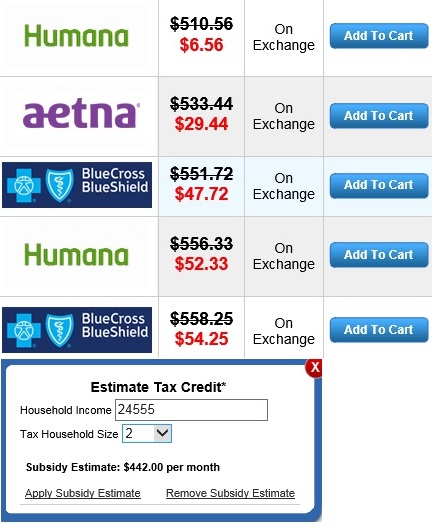
If you live in Mississippi, you can click on this calculator below to figure out your subsidy and shop for Health Insurance.
(If you have No Income or under $200 a week, click here to see some options.)
*All assistance provided is no cost to you. Purchasing a plan through Obamacare / the Federal Exchange is not the best option for everyone. A Health Insurance Plan Comparison and Consultation will be the best way for individuals and families to find affordable Mississippi health insurance and see all their options.
NOTICE: It is important to understand the ACA eliminates medical underwriting. A person’s height and weight or pre-existing conditions do not affect one’s health insurance premium.
Check status of your Ambetter Health Insurance. Let us confirm your 2023 enrollment and assist with ongoing support.
As Federally Facilitated Marketplace agents we can assist with:
Now is the time to secure your Coverage! We are here to assist with shopping, enrolling or renewing your 2023 Health Insurance:

