The Health Insurance Exchange is now active! Open enrollment is here so all Americans can shop for affordable health insurance.
If you Earn Over $230 a week click here to review the Health Exchange Plans.
Low income, earn under $230 a week, click here for Low Income assistance.
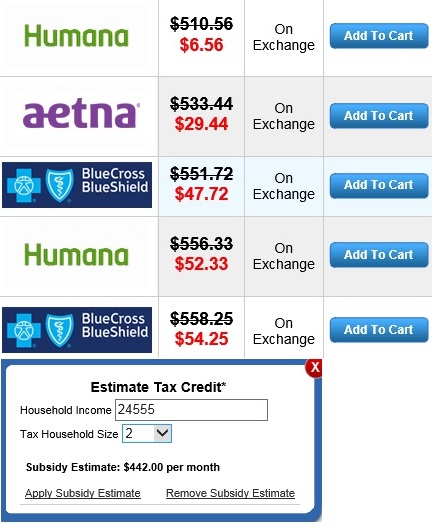
Once you select an option above, you will be able to explore plans and see if you are eligible for lower deductibles and reduced rates.
About 56% of all Americans can get Federal Money to help pay for their health insurance.