New Mexico: New Biden Plans for 2024. Lower Cost and FREE Bronze and Silver Plans! We are here to assist with shopping, enrolling or renewing your 2024 Health Insurance. Renew your plans or Sign Up Now:
United Healthcare – Blue Cross Blue Shield – Ambetter – More Options for 2024!
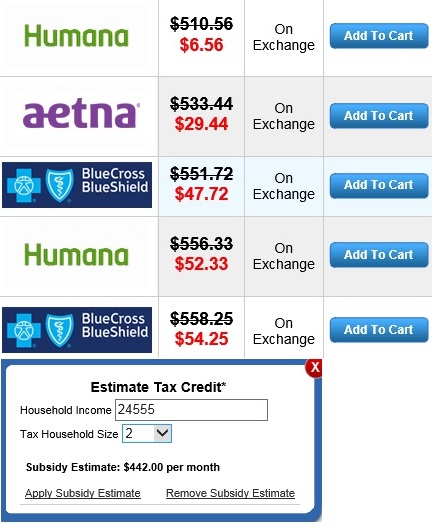
If you get a subsidy you will need help to process your application.
Once you determine your subsidy you will have to visit Help Me Get My Health Insurance Plan.
*All assistance provided is no cost to you. Purchasing a plan through Obamacare / the Federal Exchange is not the best option for everyone. A Health Insurance Plan Comparison and Consultation will be the best way for individuals and families to find affordable New Mexico health insurance and see all their options.
NOTICE: It is important to understand the ACA eliminates medical underwriting. A person’s height and weight or pre-existing conditions do not affect one’s health insurance premium.
Yes, employees in the United States can get marketplace insurance. Most job-based health insurance plans are designed for your employer to pay a portion of your monthly premium. However, if you enroll in a Marketplace plan instead, the employer won’t contribute to your insurance premium. If you have job-based insurance and want to check out options in the Health Insurance Marketplace, you can do that here. But there are several important things to know first. You can change to a Marketplace plan if you have job-based coverage now, but you probably won’t qualify for a premium tax credit or other savings. As long as the job-based plan is considered affordable and meets minimum standards, you won’t qualify for savings. The Chart below will give you more information.
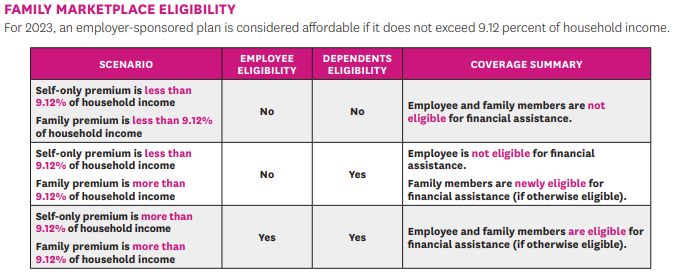
A new ACA rule fixes the Marketplace “Family Glitch”– Increasing the number of individuals eligible for Marketplace coverage in 2023. Until now under the Patient Protection and Affordable Care Act (ACA), employer offered coverage was considered affordable for all family members to whom an employer’s offer extends if the premium for the employee’s self-only coverage was considered affordable. The premium required to cover family members was not considered in deciding on subsidy. However, beginning plan year 2023, if an employee is offered employer coverage that extends to their family members, the affordability of employer coverage will be based on the family premium cost, not the Employee only premium cost. Family members will be eligible for financial assistance on the Marketplace if the employee’s family premium cost is considered unaffordable.
OPTIONS FOR COVERING THEIR FAMILY ● Split Coverage (Employer and Marketplace): Employee could enroll in the affordable employer coverage, while their family members enroll in a Marketplace plan with APTC/CSRs if otherwise eligible. ● Employer Coverage Only: Whole family could enroll in the employee’s offer of employer-sponsored coverage. While someone is enrolled in employer coverage, they aren’t eligible for financial assistance on a Marketplace plan. ● Marketplace Coverage Only: Employee could decline the affordable employer coverage, and the whole family could enroll in a Marketplace plan. They will pay full price for the employee’s portion of the Marketplace plan premium, while other family members’ portions would be lowered by using APTC and/or CSRs if they are otherwise eligible.
Missouri: New Biden Plans. Lower Cost and FREE Bronze and Silver Plans! We are here to assist with shopping, enrolling or renewing your 2023 Health Insurance. Get Started:
United Healthcare – Blue Cross Blue Shield – Ambetter – More Options for 2023!