If you live in Alabama you can click on this calculator below to figure out your subsidy.
(If you are low income, under $230 a week, click here to see some options.)
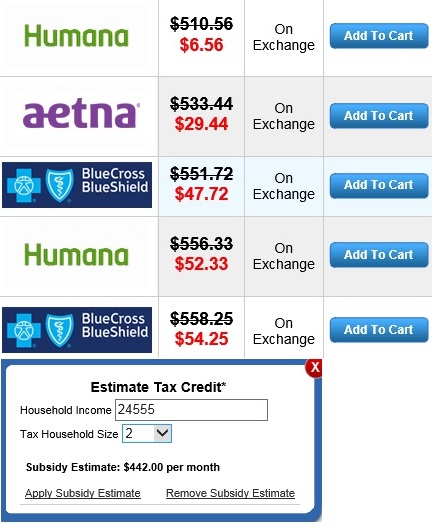
*All assistance provided is no cost to you. Purchasing a plan through Obamacare / the Federal Exchange is not the best option for everyone. A Health Insurance Plan Comparison and Consultation will be the best way for individuals and families to find affordable Alabama health insurance and see all their options.
NOTICE: It is important to understand the ACA eliminates medical underwriting. A person’s height and weight or pre-existing conditions do not affect one’s health insurance premium.








